
Services 》Calf Reduction: article
by Dr. Lih-Ren Jong
Dr. Jong is the pioneer of using shaver to reduce calf muscles. His paper has been published in the world-wide famous journal " Plastic and Reconsturctive Surgery " in April, 2020.
Dr.Jong was invited as speaker at calf reduction section in 2020 International Annual Meeting of Taiwan Society of Aesthetic Plastic Surgery.
Dr. Jong presented his experiences on calf reduction on 2017 Annual Congress of Taiwan Society of Aesthetic Plastic Surgery.
Thick muscular legs are a common aesthetic problem for Asian women. The Chinese use the term "radish-like leg" to describe the problem. Comparing with Caucasians, Asian women are relatively shorter. Women with "radish-like legs" look shorter or more obese than they really are because of their thick legs. They are embarrassed to show their legs in the summer time. Many men feel that legs are an important point of attraction, not less than breasts.
The cause of "radish-like legs" in Asians is usually calf muscle hypertrophy (excessive development), in stead of fat accumulation. This is different from protruded abdomen, buttocks, and thighs, which are often due to increased fat accumulation and can therefore be effectively treated with liposuction. However, liposuction is ineffective to treat calf muscle hypertrophy because the problem is the muscle, not fat. Doctor and Professor Ing Gon Kim in Seoul, South Korea, is a pioneer of calf reduction using small incisions and partial excision of leg muscles. In 1999, Dr. Lih-Ren Jong, director of Lih-Ren Cosmetic Clinic, studied with Professor Kim and modified Dr. Kim's technique.
An overview of the anatomy and function of the calf muscles and the various techniques to treat calf muscle hypertrophy are presented below.
What is the ideal size of calves? The analysis of ideal size of legs focus on Oriental women with average 162cm height and 49 kg weight showed that the ideal circumference of calf at its widest part is 32 cm.
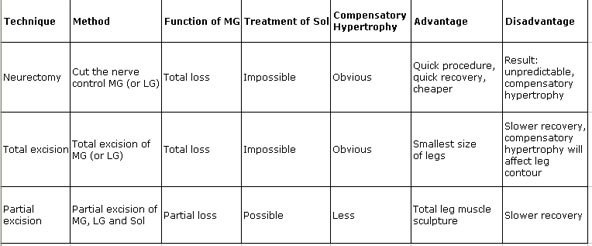
Calf reduction should consider not only the postoperative size but also the shape and function. There are three ways to reduce the size of legs: non-surgical (Botox injection ), minimal invasive way ( radiofrequency) and surgical (i.e. selective neurectomy, total excision of gastrocnemius and partial excision of gastrocnemius and Sol).
-
Anatomy and Function of Gastrocnemius
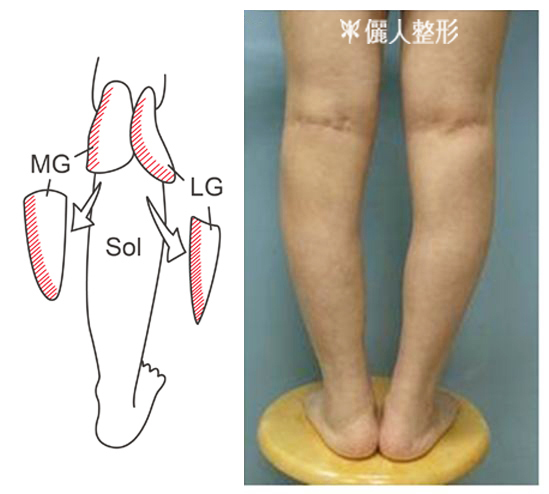
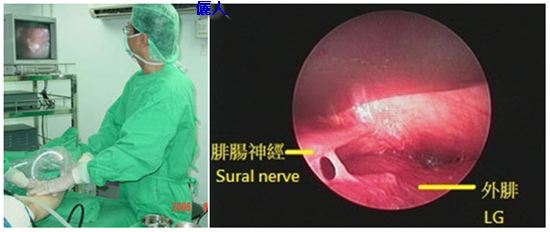
All of the leg muscles of women with radish-like legs may be hypertrophic. But the treatment of radish-like legs focus on Gastrocnemius Muscle and Soleus Muscle. Gastrocnemius is located on the superficial part of posterior calf. It is composed of medial (medial gastrocnemius, MG) and lateral head (lateral gastrocnemius, LG). Deep to the gastrocnemius is the soleus muscle (Sol). These muscles (MG, LG and Sol) share a common insertion (the Achilles tendon). The Achilles tendon is seen and felt as the strong band that points toward heel of the foot. Please refer to the figures below. MG is located in medial side of leg and is related with the medial curvature of leg. LG is located in poster-lateral side of leg. Sol is related with lateral curvature of leg. The third picture marked the location of muscles. The curve line marked the lateral edge of Sol.
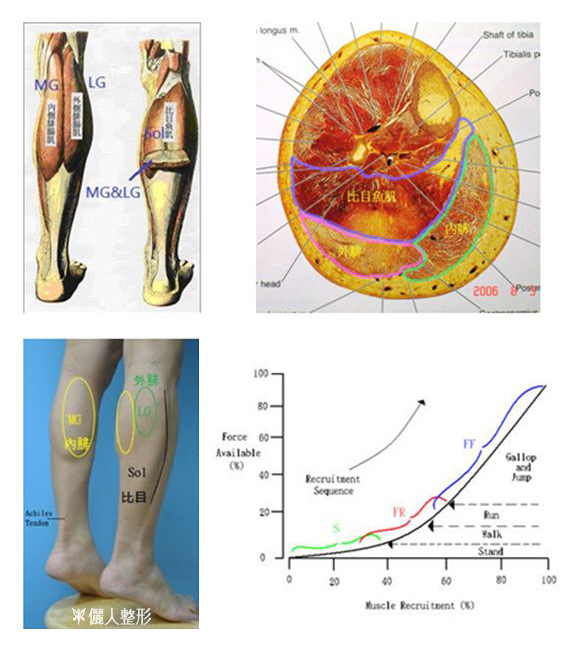
Functionally muscle cells can be divided into three types: FF cells (Fast-twitch, Fatigable), FR cells (Fast-twitch, fatigable-Resistant) and S (Slow-twitch and resistant to fatigue ) cells. Type FF cells produce large force output than type FR cells, while type S cells have uniformly small force outputs. Most of the muscle cells in MG are FF cells, but Most of the muscle cells in Sol are S cells. The attached picture shows that different cell types are recruited in different actions. In standing, the S cells in MG (including S cells in Sol ) are recruited. In walking and running, FR cells are recruited. Type FF cells in MG are required for movements that demand near-maximum force output, such as gallop or jump. In another words, Sol plays a major role in standing. MG plays a major role in gallop and jump. Sol and gastrocnemius are not functionally identical. After calf reduction operation, the function of MG will be lost partially or totally. Sol will get hypertrophic in some degree (compensatory hypertrophy) to replace the lost function of gastrocnemius. In fact, the compensatory Sol can not replace all of the lost function of gastrocnemius. If you are active in taking exercise involving legs, after operation your score will be affected in some way. Additionally the compensatory Sol will affect the final appearance of legs. Calf reduction surgery is not indicated for women who are active in taking exercise.
The loading of weight on legs are higher for obese people. The leg muscles will get thicker to provide the necessary power of movement. Our recommendation is that it is better to lose weight before calf reduction surgery. -
Botulinum toxin injection
It is a non-surgical way of calf reduction. The leg muscle will shrink in size after injection. The advantages are no scars, quick recovery. But the disadvantages are short effct( about 6 months) and minimal change in size. It is not cost-effective.
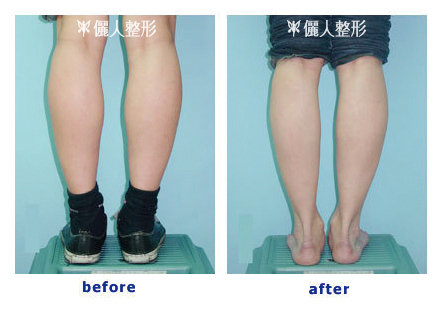
Above picture showed the result of botulinum injection . Right picture was taken on one month. Leg size reduced from 33 cm into 31 cm.
-
Selective Neurectomy
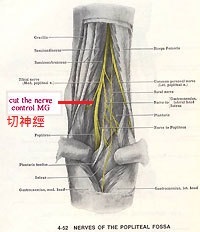
The meaning of selective neurectomy is to cut the nerve which controls the Gastrocnemius. After neurectomy, the surgeon expects Gastrocnemius to shrink in size. Some surgeons will cut the nerve of MG, LG and Sol. The more nerves cut, the slimmer the legs. But more functional disturbance on legs after the operation.
The advantage of selective neurectomy includes a quicker procedure, and it is less invasive. The major disadvantage of neurectomy is that the amount of volume reduction and the shape of legs following neurectomy is unpredictable. Muscles may grow back afer neurectomy.
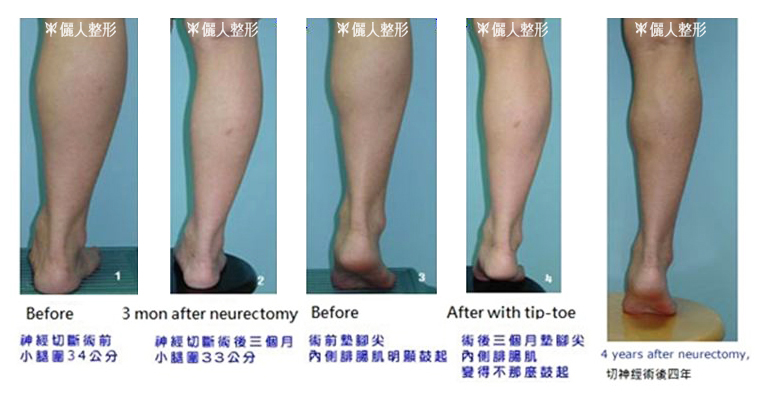
Above was an example of a patient following neurectomy. MG bulge improved when she stand on her toes 3 months after the operation. However, the patient felt that the results were inadequate since her calf circumference reduced by only 1 cm. She noted that the muscle (MG) bulged out agin 4 years after neurectomy.
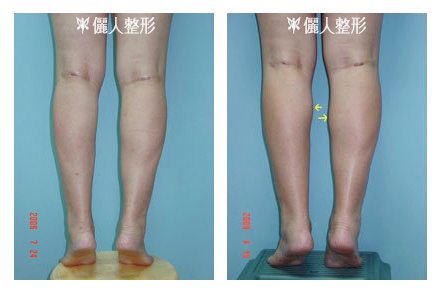
One year after neurectomy of MG, MG shrunk in size ( upper left figure). But 4 years later, bulges (arrow in upper right figure) were noted.
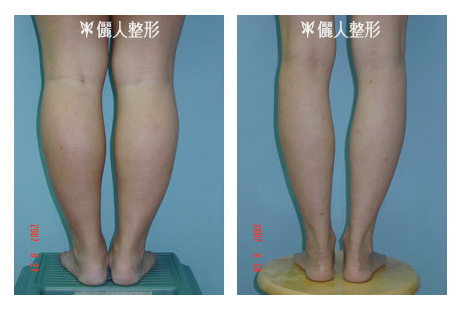
The above case underwent neurectomy 9 years ago at another clinic. You can see the obvious depression on her left leg. The muscles shrunk quite differently at her both legs after neurectomy.
The other disadvantage of neurectomy is compensatory hypertrophy of the remaining calf muscles which has been mentioned before.
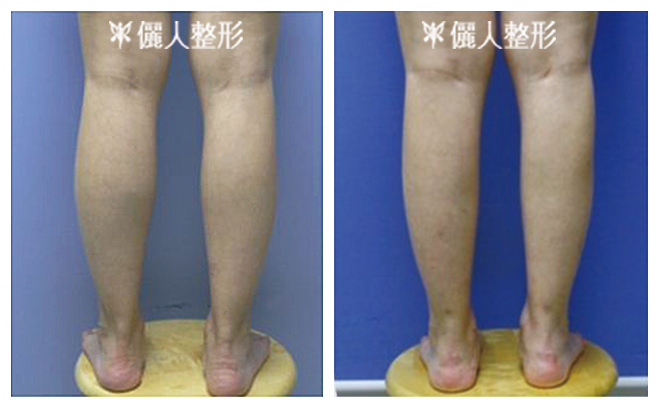
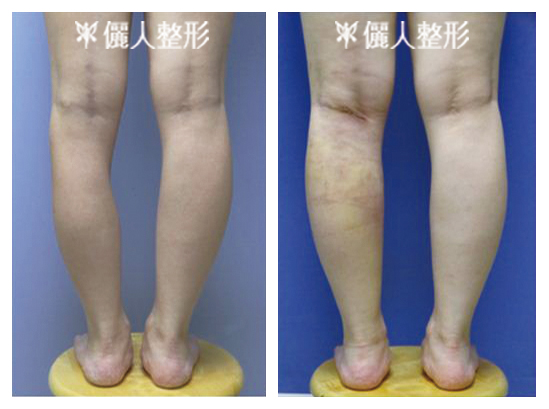
The above case underwent neurectomy in another clinic three years ago. After operation, the MG shrunk in size. But because of compensatory hypertrophy of LG and Sol, the calf bulged out in lateral side (hypertrophy of Sol) and lateral-posterior side (hypertrophy of LG).
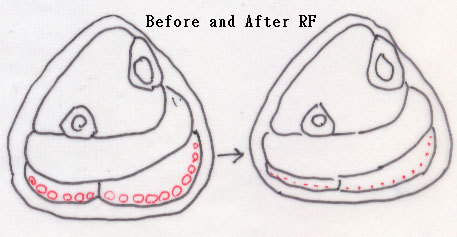
Below illustrations showed the effect of neurectomy on the cross section of legs.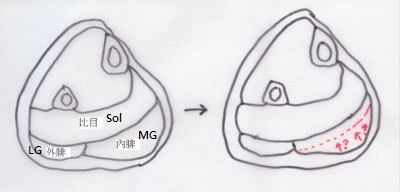
The above illustrations showed that how MG shrunk in size was unpredictable.
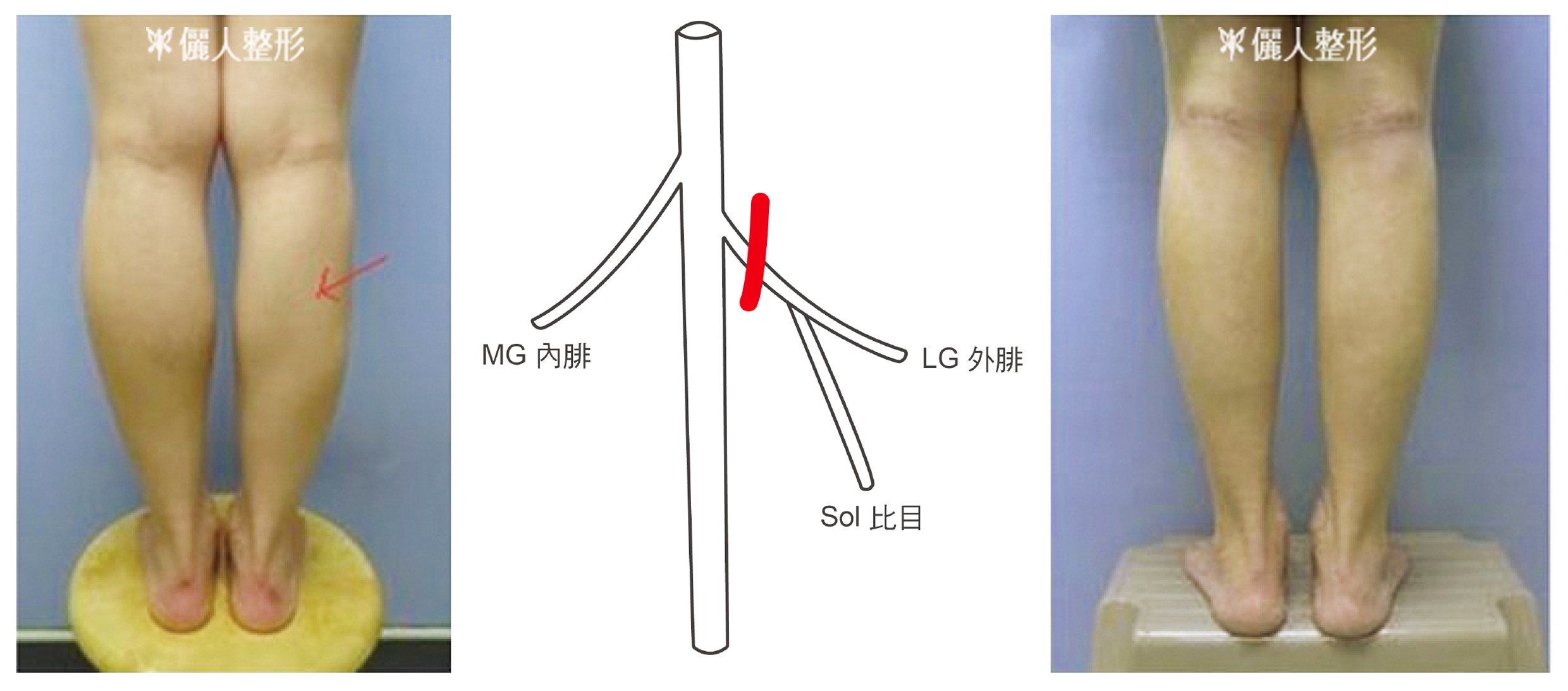
The above illustrations showed that after neurectomy of MG the compensatory hypertrophy of LG and Sol will change the contour of legs.Below demonstrated one of the complications of neurectomy. She underwent neurectomy at another clinic 4 years ago. She said that her legs grew back in half a year after surgery. The operation did not change her left leg. On her right leg, not only some parts of right gastrocnemius was thinner, but also right soleus. That caused depression on her right upper lateral leg (red arrow in below left picture). There was 2.5 cm difference between her legs. The cause of atrophic right Sol is that nerve which control Sol ( labeled " S" on the middle picture) originates from nerve to LG (labeled "L"). If cut is made on red line on the picture, LG and Sol will be shrunk. At my clinic, the bulge parts of both legs were excised. Right picture showed the postoperative result.
-
Total Excision of Gastrocnemius
Intuitively the legs will get smallest after total excision of gastrocnemius. But we emphasize that contour is more important than size. Comparing with leg muscles of women with slim legs, the leg muscles of women with radish-like legs are thicker.
Therefore surgeons have to do is to thin the muscles, in stead of taking all of them away. The legs are composed with many muscles. Could you image the contour of legs if you loss one or two major leg muscles (MG and LG)? The contour of legs after total excision of gastocnemius will be unnatural.
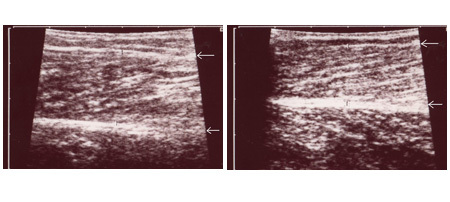
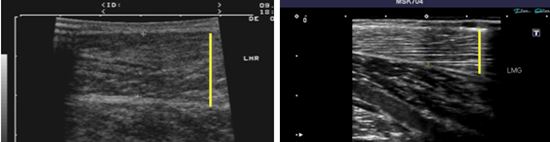
The circumference of legs of left woman is 38cm. The MG (between two arrows) thickness, measured by ultrasound, is 2 cm. The circumference of right woman is 32cm. The MG thickness is 1.6 cm. If the left woman wants to slim her legs to ideal size, similar to right woman, is it necessary to excise all of her MG ?
Operation method: the below right figure showed how total excision of gastrocnemius was performed. The below half of MG and LG was excised and preserved the upper third. The reason of preserving upper half is to decrease the hollowing below the knees after operation. Below right showed a case operated at another hospital. The depressed below medial knees were quite obvious, so that shape of legs is weird.
-
Partial Excision of Muscles (Muscle Sculpture)
The basic principle of the treatment is to selectively excise part of muscles (MG,LG and Sol) to thin the muscles. The muscles are excised pierce by pierce till the ideal shape is achieved. The surgeon sculpts the leg similar to an artist sculpting a piece of art. This is why this procedure is named "muscle sculpture". The average weight of MG is 250 gm. Depending on the severity of calf muscle hypertrophy and patient's expectation, 40 to 120 gm of muscle of MG is excised to achieve the ideal shape of medial calf. The philosophy is quite different from the other procedures mentioned above (neurectomy and total excision). There are many kinds of leg shapes, such as LG and Sol are thick in some people. Surgeons can choose to excise more LG and Sol in those cases. It is kind of custom made surgery.
The study of Professor Kim showed that ankle power returns to its preoperative level at 6 months to one year after operation.
Above is the bird-eye view comparison between before and after operation (calf reduction by partial excision of MG, LG and Sol).
Partial Excised Muscles Still KeepTheir Function?
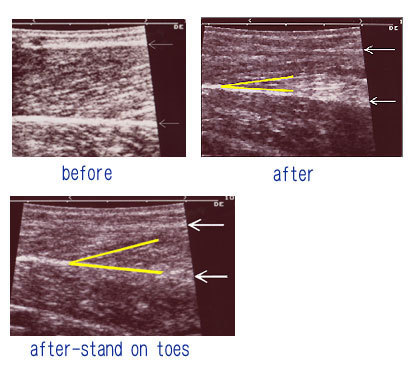
The preoperative circumference of the below case was 33cm. After partial excision of MG, LG and Sol, the circumference reduced to 29.5cm, measured two and half months after operation. The preoperative thickness of MG was 19mm (the muscle between two white arrows is MG). After surgery, it was reduced to 11 mm. When muscles contract, the fiber angle (the angle between two yellow lines) become greater. The fiber angle of relaxed MG after surgery was 12 degree. The fiber angle of contracted MG (when patient stands on toes) after surgery was 20 degree. It means that the MG muscle was still functioning after surgery in this case. It is the reason why compensatory hypertrophy is less likely to occur after muscle sculpture. (partial excision of muscles). The muscle may lose contraction function if more muscle was excised, but size of leg can be smaller.

Muscle Sculpture of Calf Muscles
The basic principle of muscle sculpture can be used not only in MG, but also in other calf muscles, such as LG or Sol. MG is related with the curvature of medial calf. MG and LG are related with the curvature of post calf. Sol is related with the curvature of lateral calf. The Sol can be trimmed without sequelae. Using concept of muscle sculpture, we can sculpt part of MG, LG or Sol . If the fat of the calf or thigh is too thick, we can also perform liposuction at the same time to sculpt the entire lower limbs.
Below illustration showed how muscle scupture worked.

When MG was partially excised but LG was not treated, LG would seem to bulge out. Usually we will recommend patients to treat MG, LG and Sol at the same time.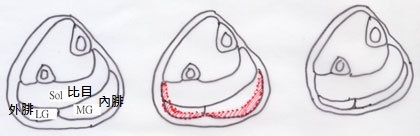
After partial excision of MG, LG and Sol, the legs can be reduced to better shape and size.
Procedure of Muscle Sculpture
The operation is usually done under spinal anesthesia. The wounds (about 4-5 cm in length) are located on the posterior side of knees. Your legs would feel nothing the operation. It takes about 5 hours to do the operation. We will insert drains into the wounds and they will be removed about 2 days later to prevent the occurrence of hematoma (blood accumulated under the leg skin).
Preoperative Preparation:- Prepare high-heels (about two inches high with board base), loose pants, prepare staying in clinic for 2 nights.
Postoperative Care:- We recommend patients to take a complete bed rest for three days. Go out of bed to rest room in 3-5 days . After 5 days, patients can start to walk.. We recommend patients not to walk too much in the first two weeks. Wearing high-heel will be more comfortable (about 2 inches high with broad base) in the early period after surgery. When feeling better, patients are recommended to wear flat shoes.
- Compression stockings can decrease leg swelling. We recommend patients to wear compression stockings for six months.
- In first three months, patients would feel tight on posterior legs. Stree exercise on ankle is important to release the contraction on posterior legs. Please follow physician instruction to do ankle exercise.
- After wounds are healed, we recommend patients to tape the scars. The scars will take more than half an year to fade out.
- When depression or irregularity are noted on leg, Message on site is recommended.
Possible Complications:Dr. Jong has performed the operation since 1997. The possible side effects are:
- Numbness on lateral foot. There is a long sensory nerve ( named sural nerve) which is located on surface of MG or LG and runs all the way from knee to lateral foot. The nerve may be injuried in the surgery. Patients may feel numb on lateral side of foot. Presently the operation is guided under endoscope. The chance of sensory nerve is lower than before ( blind operation). (please see the below figure).
- Irregular surface on legs when the surgery left with irregular surface on muscles. Under endoscope guided calf reduction, the surface of muscles can be well seen and well sculptured.
- Asymmetric. Usually there will be some asymmetric in size of legs before operation. Probably there will be some asymmetric (but not obvious) between the sizes of legs after surgery.
- We never experience cases who can not walk due to surgery.
- The MG or LG that are not excised in the surgery may be trainable and grow back. So that it is high recommended not to run or jump after surgery if patients want to keep good result.
- Hematoma (blood accumulation inside the leg) may be noted after surgery. Needle aspiration and compression would help to resolve hematoma.
Dr. Jong developed instruments to facilitate the operation. Under endoscope guide, complications were reduced. The attached picture show endoscope view of sural nerve and LG.
-
RF (radio-frequency) calf reduction
There is another way of calf reduction by RF. So called "mini-invasive calf reduction". RF is a kind of machine with probe. The probe penetrated the skin by small wounds. The RF machine generated energy to burn the small nerve in the muscle or directly burn the muscles. The muscles would shrink in size or necrotic and later on fibrotic (shown in the below-left figure). So that the thickness of muscles would be thinner. The philosophy of RF is the same as partial excision surgery. But RF is a blind method and operator can see the result during the surgery. How to control the energy and location of treatment is a challenge. Sural nerve might be damaged in the process. MG depression might be found (please see the below-right figure, arrow pointed to the depression on MG).

Below is a case presented in "Aesthetic Plastic Surgery" journal in 2013. Her left heel could not touch the floor due to contraction of left calf after RF therapy. In this paper the authors experienced the other 11 cases and stated that the effect of RF lasted more than 1.5 years after tretment. RF treatment is not so invasive as previously thought.

-
Long-Term Follow Up
Case 1,
Below case underwent calf reduction by excising the bulge on MG only 13 years ago. Below right was the picture after 13 years. The result keeps well.

Case 2,
The below male did not like the bulge on his medial calves. The bulge part of MG was excised. Below right picture was taken on six years after surgery. The result keeps well.

Below is the ultrasound pictures of his MG. The thickness decreased ( marked with yellow lines). Below right was after ultrasound picture.
Case 3,
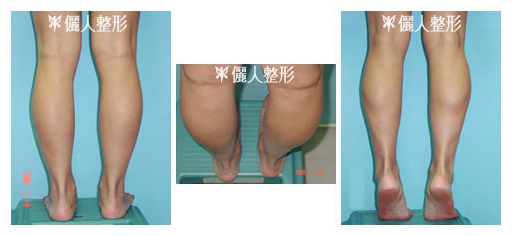
Below left picture was before picture. Middle was taken on 9 mon after calf reduction by partial excision of MG, LG and liposuction of her legs. Her leg size was reduced from 41 cm to 36 cm. The change was quite dramatic. Below right was taken on 7.5 years after surgery. In the past days, she exercised very much to lose weight. Bulges were noted again on her legs, especially on left leg. Because the muscles may be trained, it is recommended not to run or jump after surgery.

-
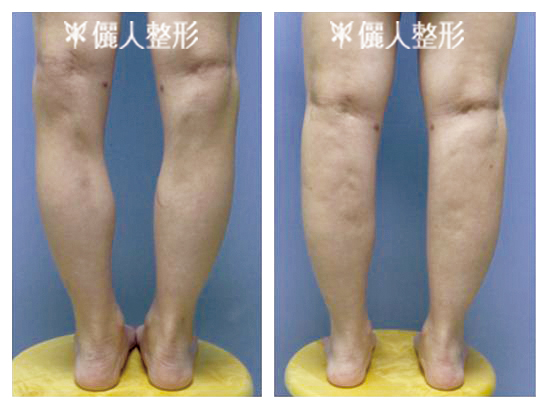
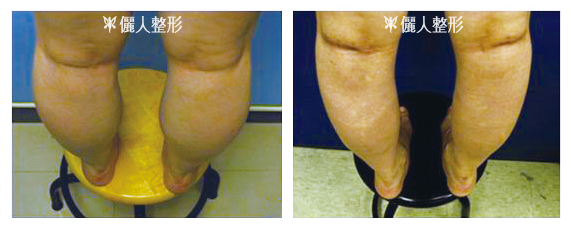
If you live abroad and are interested in calf reduction, you may write down the questions you have. Take the pictures of your legs (pictures of back view of your legs and picture of legs standing on toes) following the same way as the below examples. Measure the circumference of your legs at their widest part and e-mail to: mail@LRclinic.com.tw We will reply as soon as possible.

If you live abroad, you may send your questions and pictures (such as eyes, etc) to mail@LRclinic.com.tw .
We will reply you as soon as possible.








